

Diaphragm and abdominal breathing: when "breathing with the diaphragm" is the problem, not the solution
Mauro Lastrico, Giuseppe Macrì – Physiotherapists
Abdominal breathing observed in many patients may be the sign of muscular shortening preventing costal expansion — not the sign of good diaphragmatic breathing. The diaphragm has four points of action: two on the ribs and two on the spine. When costal expansion is blocked, the diaphragm acts on the vertebral crura, increasing lumbar lordosis and compressing the intervertebral discs. The diaphragm does not need re-education but freeing.
This article presents the biomechanical analysis of the thoracic diaphragm within the AIFIMM analytical and systemic model, integrated with the functional considerations of Dr. Giuseppe Macrì, physiotherapist
The diaphragm in the sagittal plane: the diaphragm-psoas force couple
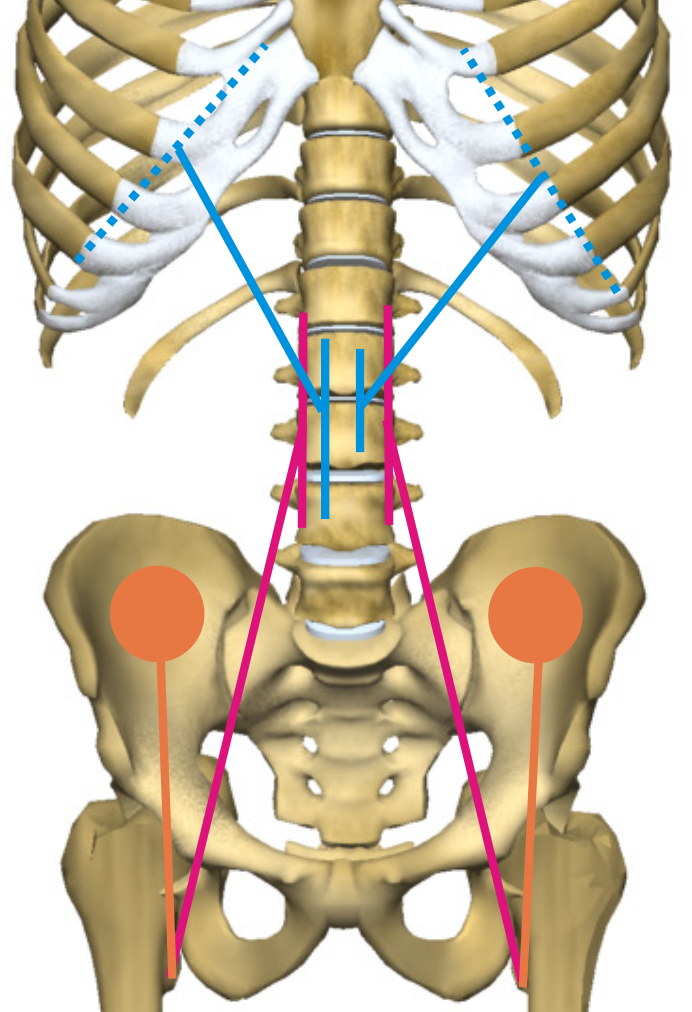
The diaphragm crura insert on the lumbar vertebrae from L1 to L4. The psoas inserts from T12 to L4. Together they form a force couple that pulls the lumbar vertebrae anteriorly — the diaphragm toward the thorax, the psoas toward the femur. This couple is one of the principal motors of lumbar hyperlordosis.
In the thoraco-lumbo-sacral segment, the diaphragm is not an isolated muscle: it is co-agonist of all muscles with direct spinal insertion in increasing lordosis — paravertebral muscles, quadratus lumborum, latissimus dorsi, psoas. The rectus abdominis muscles, the only antagonists, are subdominant.
The vertical components of the oblique forces of the diaphragm crura sum bilaterally with those of the other muscles with spinal insertion, producing stiffening of the lumbar segment and disc compression. Shortening of the crura directly contributes to compression of the intervertebral discs from L1 to L4.
The diaphragm in the frontal plane: lumbar convexity
When shortening of the diaphragm crura is asymmetric, the direct traction on the L1–L4 vertebrae produces homolateral lumbar convexity. The diaphragm, together with the psoas and quadratus lumborum, may oppose the mechanical resultant of hemipelvic elevation or add to it, producing the apparently incongruent patterns described in the frontal plane vector analysis.
A muscle with four legs: the respiratory mechanics of the diaphragm
The diaphragm can be understood as a muscle with four points of action beyond the central tendon: two on the lower ribs and two on the spine — the vertebral crura.
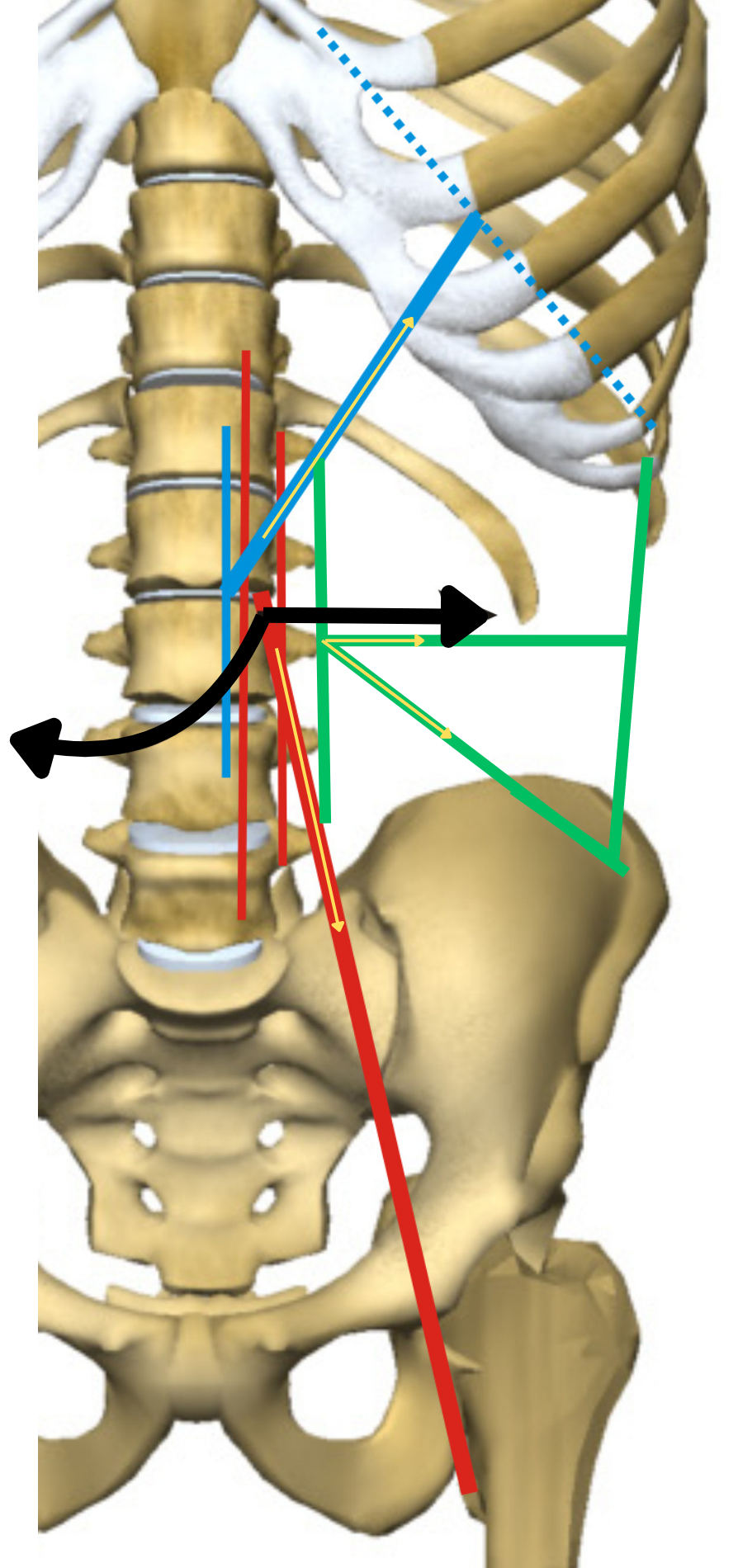
In physiological inspiration, the diaphragm acts on the costal insertions. The central tendon descends, then the costal insertions expand the rib cage laterally. The increase in thoracic volume occurs at zero vertebral cost: the spine is not involved.
But if costal expansion is impeded — for example by shortening of the latissimus dorsi or the obliques — the diaphragm must still guarantee inspiration. Respiratory function is a priority: the "what" prevails over the "how."
In this case, the diaphragm changes strategy: instead of acting on the ribs, it acts on the vertebral crura. Together with the psoas, with which it forms a force couple, it lifts the thorax by increasing lumbar lordosis. The vertebrae from L1 to L4 are pulled anteriorly, the intervertebral discs undergo compression, and the abdomen "inflates" as the mechanical resultant of the anterior projection of the thoraco-lumbar spine.
This is an emergent ability: a substitutive strategy that the system develops to maintain a priority function at the expense of the spine. The abdomen inflating during inspiration is not the sign of "good diaphragmatic breathing" — it is the sign that the diaphragm is using its crura instead of its ribs, and that the spine is paying the price.
Direct clinical consequence
So-called abdominal breathing observed in many patients may be the sign of shortening of the latissimus dorsi and obliques that prevents costal expansion — not a deficit of the diaphragm. Re-educating breathing without freeing the thorax from the shortening of the muscles that prevent its expansion is futile: the diaphragm will continue to use the crura because it has no alternative.
In the AIFIMM model, the diaphragm does not need to be re-educated but freed. The substitutive respiratory strategy resolves when the causes preventing costal expansion — shortening of the latissimus dorsi, obliques, lower trapezius fibres — are treated. Only then can the diaphragm return to acting on the ribs instead of on the spine.
Diaphragm and visceral correlations
The diaphragm separates the thoracic cavity from the abdominal cavity and has direct relationships with the heart (through the phrenic-pericardial ligament), oesophagus, aorta, and vena cava. The viscero-somatic correlations of the T10–L2 segment connect the diaphragm crura to the adrenals, kidneys, and ureters.
A visceral dysfunction in these districts may maintain tension on the diaphragm crura through neurological organ-vertebra connections. If direct muscular treatment produces temporary improvements but respiratory dynamics and lumbar lordosis return to the previous condition, this is the clinical signal of secondary shortening: the primary cause is visceral and the diaphragm is adapting.
The diaphragm, because of the primary function it serves, must continuously adapt to alterations imposed by adjacent structures. When it can no longer transfer these distortions, symptoms appear — intercostal pain, cervico-dorsal or dorso-lumbar pain, and respiratory dysfunctions that do not have a pulmonary origin.
This article is part of the AIFIMM biomechanical model. See the complete list of articles. Download the free introductory e-book.
The diaphragm as a polyfunctional muscular complex — Dr. Giuseppe Macrì
The diaphragm is a digastric muscular complex, formed peripherally by flat muscle bellies arranged radially and centrally by overlapping tendinous and aponeurotic bands of connective tissue. The bilateral trigones distinguish the contractile fibres into three portions — sternal, costal, and vertebral — with functional significance linked to the different dynamics of the osteoarticular structures on which they insert. Myofibrils range from short in the sternal portion to more than double in the costal portion.
The pericardial pivot point
The diaphragm has a suspension system through the phrenic-pericardial ligament anchored to the central tendon, where the fusion of the fibrous elements of the pericardial sac with the central tendon becomes intimate. In static breathing, the diaphragm uses this tendinous anchorage as a pivot point — the most energy-efficient solution that does not shift the body's centre of mass forward.
This intimate relationship between pericardium and diaphragm is characteristic of humans: it is the evolutionary consequence of the transition from the horizontal stance of quadrupeds to the upright stance. In animals where the heart rests on the sternum, this relationship does not exist.
Pressure homeostasis and posture
The diaphragm contributes to posture through the maintenance of alternating intracorporeal pressure homeostasis between the thoracic and abdominal cavities. Without it, standing upright would require enormous energy expenditure. The diaphragm complex compacts the trunk and abdomen, solidarising the spine — a synergism between container and contents in which the pelvic diaphragm also plays a fundamental role.
Only during intense physical effort does the diaphragm need additional abdominal counterforce from the rectus abdominis, transversus abdominis, and pelvic diaphragm. Individuals who maintain abdominal hyperpressure even at rest force the diaphragm to compensate for the functional asymmetry, discharging tensions at the dorso-lumbar level with consequent pain syndromes that may eventually structure at the osteoarticular level.
A muscle that can never rest
The diaphragm is the only striated muscle that can never rest. It must always be ready to execute protective actions — sneezing, coughing, vomiting — produce the airflow for phonation, contribute to the maintenance of posture, and create the thoraco-abdominal block for limb movement. For this reason, it must continuously adapt to mobility alterations imposed by adjacent anatomical structures, using even sectoral structural compensations.
This topic is part of the online course Systemic and Segmental MSK Biomechanics.
References
[1] Neumann DA. Kinesiology of the Musculoskeletal System. 3rd ed. St. Louis: Elsevier; 2017. [2] De Troyer A, Estenne M. Coordination between rib cage muscles and diaphragm during quiet breathing in humans. J Appl Physiol. 1984;57(3):899-906. [3] Hodges PW, Gandevia SC. Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J Appl Physiol. 2000;89(3):967-976. [4] Hodges PW, Heijnen I, Gandevia SC. Postural activity of the diaphragm is reduced in humans when respiratory demand increases. J Physiol. 2001;537(Pt 3):999-1008. [5] Kolar P, Sulc J, Kyncl M, Sanda J, Neuwirth J, Bokarius AV, Kriz J, Kobesova A. Postural function of the diaphragm in persons with and without chronic low back pain. J Orthop Sports Phys Ther. 2012;42(4):352-362. [6] McGill SM. Low Back Disorders: Evidence-Based Prevention and Rehabilitation. 3rd ed. Champaign: Human Kinetics; 2016. [7] Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain. Clin Biomech. 1996;11(1):1-15. [8] Adams MA, Dolan P. Spine biomechanics. J Biomech. 2005;38(10):1972-1983. [9] Bordoni B, Zanier E. Anatomic connections of the diaphragm: influence of respiration on the body system. J Multidiscip Healthc. 2013;6:281-291. [10] Bordoni B, Marelli F, Morabito B, Sacconi B. The indeterminable resilience of the fascial system. J Integr Med. 2017;15(5):337-343. [11] Barral JP. Visceral Manipulation. Vol. 1 and 2. Seattle: Eastland Press; 2005. [12] Bogduk N, Pearcy M, Hadfield G. Anatomy and biomechanics of psoas major. Clin Biomech. 1992;7(2):109-119. [13] Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis: Mosby; 2002. [14] Winter DA. Biomechanics and Motor Control of Human Movement. 4th ed. Hoboken: Wiley; 2009. [15] Mead J, Agostoni E. Dynamics of breathing. In: Fenn WO, Rahn H, editors. Handbook of Physiology: Respiration. Washington: American Physiological Society; 1964. p. 411-427. [16] Giamberardino MA. Referred muscle pain/hyperalgesia and central sensitisation. J Rehabil Med. 2003;(41 Suppl):85-88.