

The iliopsoas: why it shortens, why stretching fails, and what to do instead
Mauro Lastrico, Giuliano Chiri – Physiotherapists
The most widespread exercise for lengthening the iliopsoas — hip extension in a rear lunge — is a biomechanical misconception. The psoas inserts from T12 to L4: when the femur extends, the lumbar spine cannot be fixed because all muscles with direct spinal insertion are co-agonists in increasing lordosis. The femur goes backward, the spine goes forward, and the psoas is not lengthened. The result is disc compression and vertebral rotation at the expense of the lumbar spine.
This article presents the biomechanical analysis of the iliopsoas within the AIFIMM analytical and systemic model, integrated with the anatomical and visceral work of Dr. Giuliano Chiri, physiotherapist and AIFIMM instructor.
The iliopsoas in the sagittal plane: co-agonist in increasing lordosis
In the thoraco-lumbo-sacral segment, all muscles with direct spinal insertion are co-agonists in increasing lordosis. The psoas, with its insertions from T12 to L4, pulls the lumbar vertebrae anteriorly toward the femur. The diaphragm, through its crura with insertions from L1 to L4, pulls the vertebrae anteriorly toward the thorax. Together they form a force couple that projects the lumbar spine forward.
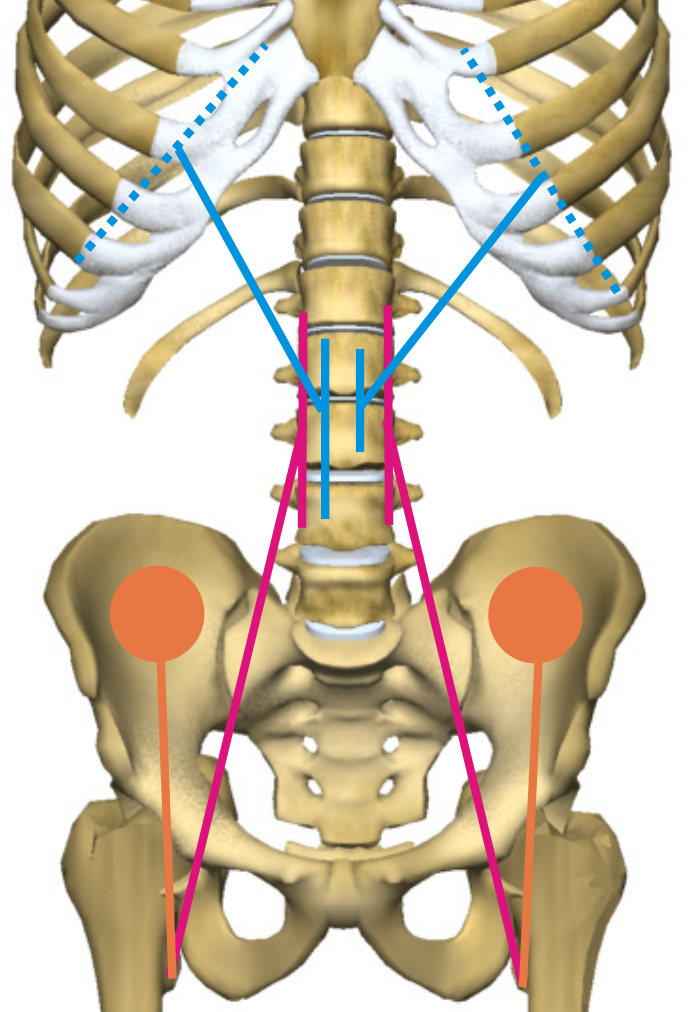
To these are added the paravertebral muscles, quadratus lumborum, and latissimus dorsi posteriorly, and the iliacus with anterior pelvic tilt. The only antagonists — the rectus abdominis muscles — have no direct spinal insertion and are vectorially subdominant.
Equilibrium is highly unstable: even modest shortening of the psoas produces modification of the thoraco-lumbar curve and compression on the intervertebral discs. The vertical components of the oblique forces of the psoas sum bilaterally with those of the paravertebral muscles, producing stiffening and disc compression.
The iliopsoas in the frontal plane: lumbar convexity
When psoas shortening is asymmetric, its direct traction on the L1–L4 vertebrae produces homolateral lumbar convexity. This action may oppose the mechanical resultant of hemipelvic elevation — produced by the latissimus dorsi and quadratus lumborum — or add to it.
When the quadratus lumborum, diaphragm, and psoas act in synergy, they maintain the lumbar spine vertical or deviate it homolaterally even in the presence of an elevated hemipelvis. This explains apparently incongruent patterns in which the lumbar vertebrae are in homolateral convexity relative to the elevated pelvis: it is not an anomaly but the predictable resultant of vectors with direct spinal insertion opposing the mechanical resultant of pelvic elevation.
The iliopsoas under load: dominance in anterior tilt
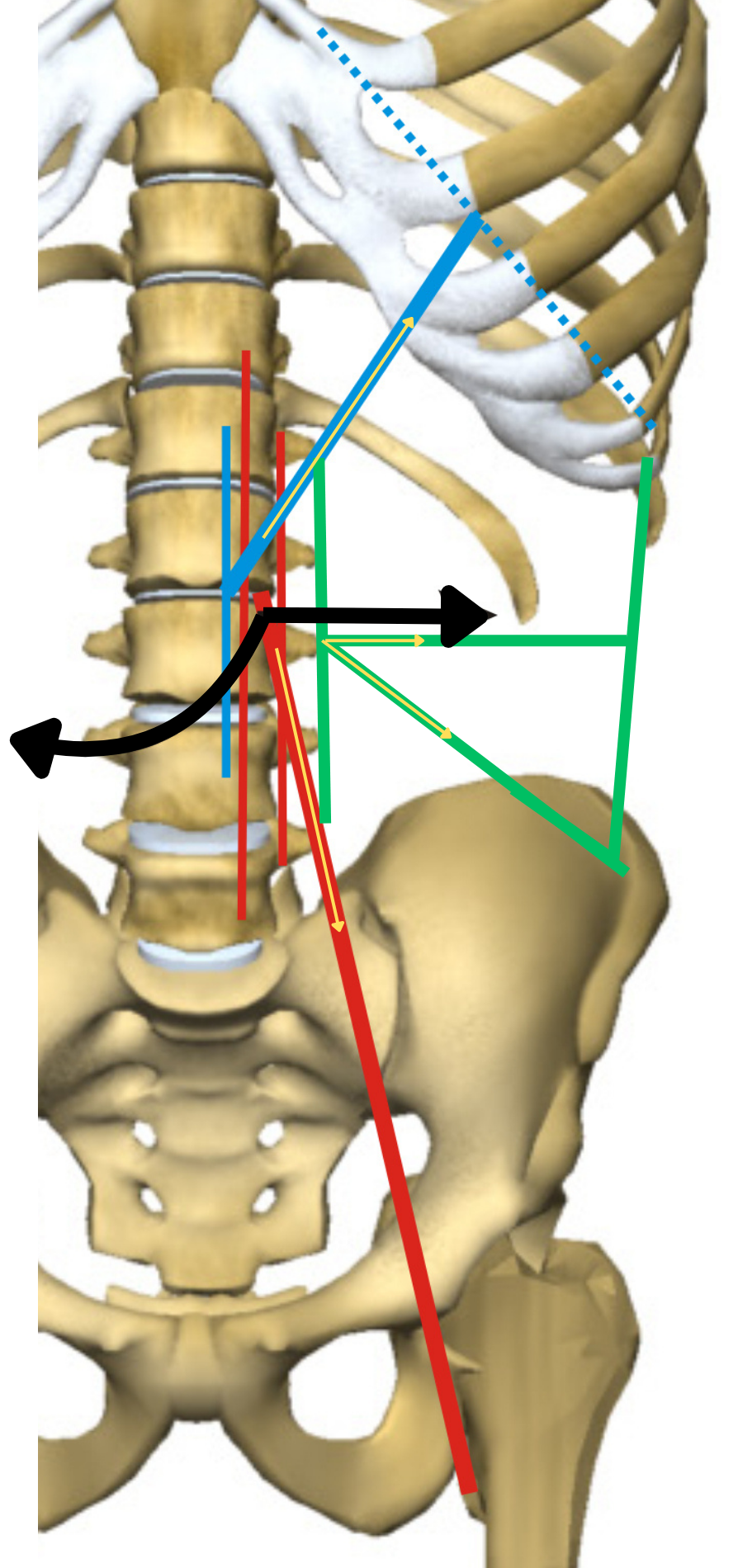
With the femur as the mobile point — unloaded — the psoas is a hip flexor. With the femur as the fixed point — under load, in standing — the same muscle changes the direction of its action: instead of bringing the femur toward the pelvis, it brings the pelvis toward the femur, producing anterior pelvic tilt and lumbar hyperlordosis.
This dominance is particularly relevant because under load the hip extensors — hamstrings and gluteals — are subdominant when axial loading increases the stabilisation required of the joint. The resultant vector dominance favours anterior tilt.
Resistant Force and Work Force in the iliopsoas
Connective shortening of the psoas produces the clinical paradox typical of the FR/FL model: the muscle opposes resistance to lengthening — high Resistant Force — but has lost the ability to contract effectively — reduced Work Force. The psoas "holds" the spine in lordosis but works worse.
Strengthening a shortened psoas does not correct the mechanical cause. The increase in Work Force is dissipated in the attempt to overcome internal Resistant Force. The result is increased disc compression. Reducing Resistant Force is the prerequisite for the psoas to recover efficiency.
Why stretching the iliopsoas is a biomechanical misconception
The most widespread exercise for "lengthening" the psoas is hip extension — the classic rear lunge. The apparent logic is simple: move the insertions apart to stretch the muscle. The problem is that this logic ignores an elementary physical condition: to lengthen a muscle, a fixed point and a mobile point moving away from it are required.
The psoas inserts from T12 to L4 and onto the lesser trochanter. When the femur is taken into extension, the lumbar spine cannot be fixed: no muscle can prevent its anterior movement because all muscles with direct spinal insertion — paravertebral muscles, quadratus lumborum, latissimus dorsi, diaphragm — are co-agonists of the psoas in increasing lordosis. There is no vertebral fixed point.
The result: the femur goes backward, the spine goes forward. The psoas is not lengthened — its vertebral insertions follow the movement. What is produced is increased lordosis with disc compression and vertebral rotation. The illusion of lengthening is created by the increase in coxo-femoral angle, but that range is gained at the expense of the spine, not of the psoas.
The usual correction makes the problem worse. To "fix" the spine, the opposite hip is flexed to bring the pelvis into posterior tilt. This apparently eliminates the lordosis but creates a greater mechanical conflict: with the pelvis in posterior tilt, the sacrum verticalises and the L5–S1 junction is subjected to a force moment that projects L5 anteriorly. The vertebrae rotate and asymmetric disc compressions increase.
In both cases — with or without pelvic posterior tilt — the psoas is not lengthened and the spine sustains mechanical damage. The error lies in the premise: treating the psoas as a muscle that can be isolated with segmental stretching, ignoring that it is part of a system of forces in which all vectors with spinal insertion are co-agonists.
In the AIFIMM model, reduction of Resistant Force in the psoas is achieved through isometric contractions performed at maximum physiological lengthening — where the lengthening point is controlled by the therapist in relation to the response of the entire system, not imposed by an exercise that the system compensates at the expense of the spine.
When direct treatment is not enough: visceral correlations
In the AIFIMM clinical reasoning model, the distinction between primary and secondary shortening is decisive. If direct muscular treatment of the psoas produces temporary improvements but the symptom recurs, this is the clinical signal of secondary shortening: the primary cause lies elsewhere and continues to require muscular adaptation.
The viscero-somatic correlations of the T10–L2 segment connect the psoas to the diaphragm, adrenals, kidneys, and ureters. A visceral dysfunction in these districts may maintain tension on the psoas through neurological organ-vertebra connections, rendering any muscular correction unstable.
It is here that the anatomical work of Dr. Giuliano Chiri — in the section that follows — provides the detailed map of the relationships between the psoas, the iliac fascia, neural structures, and visceral organs that support this clinical interpretation.
This article is part of the AIFIMM biomechanical model. See the complete list of articles. Download the free introductory e-book.
Anatomy, fascial relationships, and visceral correlations — Dr. Giuliano Chiri
Insertions
The iliopsoas is formed by two muscles distinct at their origin. The psoas major originates from the lateral surface of the body of the last thoracic vertebra and from L1 through L4. Fascicles insert on the intervertebral discs and at the base of the transverse processes of the last four lumbar vertebrae. It descends inferolaterally, crossing the lumbar and iliac regions, passes beneath the inguinal ligament, and inserts onto the lesser trochanter, passing anterior to the hip joint.
The iliacus is fan-shaped and originates from the inner lip of the iliac crest, the entire iliac fossa and its circumference, the iliolumbar ligaments, and the base of the sacrum. It inserts together with the tendon of the psoas major.
Innervation is from muscular branches of the lumbar plexus and the femoral nerve, roots L1–L4.
Anatomical relationships
The psoas major has relationships with the medial arcuate ligament of the diaphragm, the kidney, the ureter, the renal vessels, the ascending colon on the right, the descending colon on the left, and hosts the femoral nerve.
The iliacus has relationships with the caecum and appendix on the right, and the iliac colon on the left.
Relationships with the iliac fascia
Anterior to the iliopsoas extends one of the most important fasciae: the lumbo-iliac fascia. This fascia occupies the entire width of the iliac fossa transversely and extends from the superior insertion of the psoas major to its trochanteric insertion. It inserts on the entire contour of the iliopsoas.
The iliac fascia has relationships with all lumbar vertebrae, the base of the sacrum, the superior base of the lesser pelvis, the aponeurosis of the quadratus lumborum, the iliolumbar ligament, the iliac crest, the fibrous arch of the psoas major (which in turn relates to the diaphragm), and the inguinal ligament. Below the inguinal ligament, the iliac fascia accompanies the extrapelvic portion of the iliopsoas and continues into the thigh with the femoral fascia descending with the sartorius and with the fascia of the pectineus.
Neural implications
Conditions affecting the iliopsoas may involve neural structures: the lateral femoral cutaneous nerve, the genitofemoral nerve, the obturator nerve, and the femoral nerve with corresponding dermatomal involvement.
The abdominal sympathetic chain rests on the aponeurosis of the psoas. The iliopsoas may influence the sympathetic system, just as it is subject to the effects of any influence with a sympatheticotonic component. Symptomatology is explained both by the possibility of direct contact between the ganglia of the lateral vertebral chain and the psoas, and by intermediation of the orthosympathetic arterial vascular circulation.
Visceral implications
The retrorenal fascia covers the quadratus lumborum and subsequently the psoas, fixing at vertebral level. The ureter, liver, duodenum, ascending colon, caecum, descending colon, and vermiform appendix have direct relationships with the iliac fascia or with the iliopsoas.
The psoas and the sacroiliac joints are subject to frequent fixations, particularly because this muscle is innervated by lumbar nerve plexuses that also serve most abdominal organs.
According to Barral, the psoas often undergoes spasm in patients with gastro-oesophageal problems, partly because its ligaments exchange fibres with the diaphragm, and also because the sympathetic nerves crossing it may become irritated.
Renal ptosis may be accompanied by femoral nerve involvement. From a dysfunction standpoint, the psoas acts as a track along which the kidney slides caudally. This may determine homolateral thigh hypersensitivity accompanied by knee pain without prior trauma. Internal capsular pain increases on knee flexion, making kneeling or squatting poorly tolerated. The knee pain leads to spasm tending to bring the lower leg into external rotation, with a change in limb axis causing joint pain at the ankle and foot — problems of mechanical nature that are of visceral origin.
This topic is part of the online course Systemic and Segmental MSK Biomechanics.
References
[1] Neumann DA. Kinesiology of the Musculoskeletal System. 3rd ed. St. Louis: Elsevier; 2017. [2] Bogduk N. Clinical and Radiological Anatomy of the Lumbar Spine. 5th ed. Edinburgh: Elsevier; 2012. [3] Bogduk N, Pearcy M, Hadfield G. Anatomy and biomechanics of psoas major. Clin Biomech. 1992;7(2):109-119. [4] Andersson E, Oddsson L, Grundström H, Thorstensson A. The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scand J Med Sci Sports. 1995;5(1):10-16. [5] Penning L. Psoas muscle and lumbar spine stability: a concept uniting existing controversies. Eur Spine J. 2000;9(6):577-585. [6] Keagy RD, Brumlik J, Bergan JL. Direct electromyography of the psoas major muscle in man. J Bone Joint Surg Am. 1966;48(7):1377-1382. [7] Sajko S, Stuber K. Psoas major: a case report and review of its anatomy, biomechanics, and clinical implications. J Can Chiropr Assoc. 2009;53(4):311-318. [8] Adams MA, Dolan P. Spine biomechanics. J Biomech. 2005;38(10):1972-1983. [9] McGill SM. Low Back Disorders: Evidence-Based Prevention and Rehabilitation. 3rd ed. Champaign: Human Kinetics; 2016. [10] Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain. Clin Biomech. 1996;11(1):1-15. [11] Barral JP. Visceral Manipulation. Vol. 1 and 2. Seattle: Eastland Press; 2005. [12] Giamberardino MA. Referred muscle pain/hyperalgesia and central sensitisation. J Rehabil Med. 2003;(41 Suppl):85-88. [13] Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis: Mosby; 2002. [14] Winter DA. Biomechanics and Motor Control of Human Movement. 4th ed. Hoboken: Wiley; 2009. [15] Gajdosik RL. Passive extensibility of skeletal muscle: review of the literature with clinical implications. Clin Biomech. 2001;16(2):87-101. [16] Weppler CH, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 2010;90(3):438-449.